AI Health Summary for Doctor: Where Health AI Is Safe
An AI health summary for the doctor organizes what you already know without diagnosing. Here is the one framing that keeps health AI on the right side of the law.
By Mike Hodgen
The well-baby visit problem nobody designs for
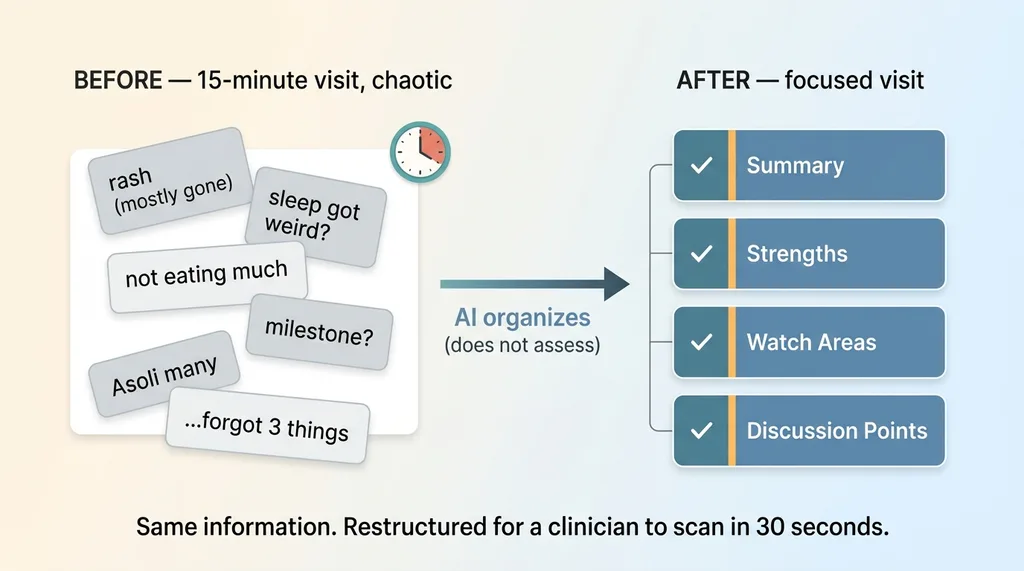
A parent walks into a 15-minute pediatric visit with a phone full of half-remembered worries. The kid hasn't been eating much. The sleep got weird two weeks ago. There was a rash that's mostly gone now. A milestone they read about online that hasn't shown up yet.
 The well-baby visit gap: chaos in, structure out
The well-baby visit gap: chaos in, structure out
They meant to ask five things. They ask two. They walk out remembering the other three in the parking lot.
On the other side of the table, the clinician gets fragmented information delivered out of order under time pressure. The rash comes up first even though it's resolved. The sleep change, which might actually matter, gets buried. There's no narrative, just a pile of observations dumped in whatever order anxiety surfaced them.
The gap here is not medical knowledge. The pediatrician has plenty of that. The gap is organization. Nobody designed a way to take what the parent already observed and shape it into something a busy clinician can use in the few minutes they actually have.
I built an ai health summary for doctor visits inside a consumer health-adjacent app. The whole point was closing that gap. Not adding intelligence to the room, just adding structure.
And the first instinct everyone has when you describe this problem is the wrong one.
The obvious move is to have the AI assess the child. Feed it the symptoms, let it suggest what might be going on, hand the parent a head start on the diagnosis. It feels helpful. It demos well.
It's also a trap. The second you point AI at a child and let it render any kind of verdict, you've built a liability, not a feature. I'll explain exactly why, and then what I built instead.
Why an AI that diagnoses is a liability, not a feature
Let me be direct about the reasons you don't let AI assess or diagnose, because they're not soft concerns.
The first is legal. An AI that tells a parent "this looks like an ear infection" is practicing medicine without a license. It doesn't matter that a model generated it. If your product delivers a clinical conclusion to a user, your product made a medical claim, and you own it.
The second is regulatory. The moment software is intended to diagnose or guide treatment, you're in FDA software-as-a-medical-device territory. That's a different universe of compliance, validation, and clearance. Most teams building a "helpful health assistant" have no idea they just wandered into it.
The third is the one that actually keeps me up. If your AI is wrong about a child, can you stand behind it? Not legally, ethically. Can you defend a verdict that a language model produced based on a parent's anxious typing at 11pm? You can't. There is no version of "the model said so" that holds up when a kid is involved.
Here's the part nobody likes to hear. A disclaimer does not save you. The instant an AI says "this looks like X" or even strongly implies a verdict, you've crossed a line that no amount of fine-print "this is not medical advice" fully walks back. The user read the assessment. The assessment is the product they remember.
This is exactly where most health AI demos go wrong. They show the model being clever about a case, and the room nods, and nobody notices they just watched an unlicensed entity diagnose a patient on stage.
I build the guardrails that keep a health AI from practicing medicine into the product itself, not as a footer. The refusal to assess the child isn't a limitation I apologize for. It's the design.
The safe sweet spot: organize, don't assess
So where is AI actually safe and valuable in healthcare? Here's the principle, stated plainly:
 Organize vs. Assess: the safe line for health AI
Organize vs. Assess: the safe line for health AI
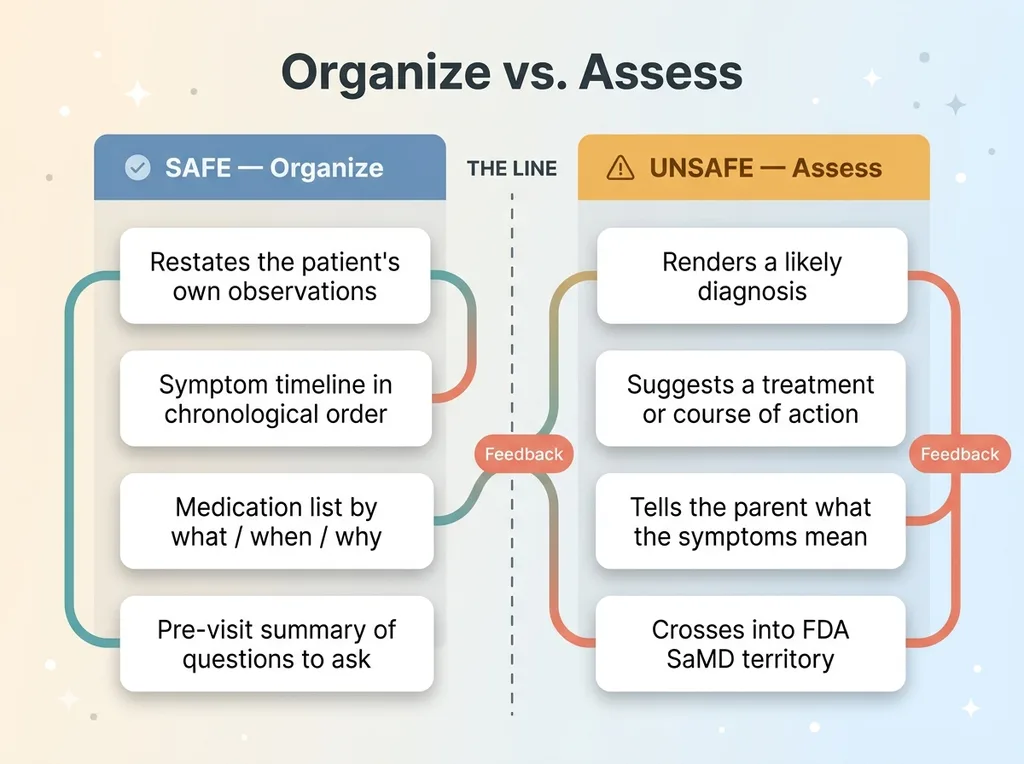
The safe place for AI in healthcare is summarizing and structuring information the patient or caregiver already provided, not generating clinical conclusions.
That's the whole line. AI is excellent at taking scattered observations and producing an ordered, readable summary. It is not good at, and should never be asked to, render a verdict about what those observations mean medically.
Think about what that distinction buys you. The parent already knows the kid hasn't been eating. They already noticed the sleep change. None of that information requires a medical license to repeat back in a cleaner form. AI organizing your own notes is not AI making a diagnosis.
This is why an ai pre-visit report is one of the safest, most useful patterns in healthtech. You're not adding clinical judgment. You're taking what the patient typed and turning it into a structured timeline a doctor can scan in 30 seconds instead of reconstructing through ten minutes of back-and-forth.
The same logic generalizes well past pediatrics:
- Medication lists organized by what, when, and why the patient takes them
- Symptom timelines that put events in chronological order instead of order-of-worry
- Pre-visit summaries that surface the questions a patient actually wants answered
All of that is patient-facing health ai that never crosses the line, because it never concludes anything. It restates and reorganizes. The intelligence is in the structure, not in a diagnosis.
Get this distinction right and you can ship something genuinely useful that no regulator and no plaintiff's attorney can credibly call practicing medicine.
What I actually built: a parent summary, not a clinical assessment
Here's the feature, concretely.
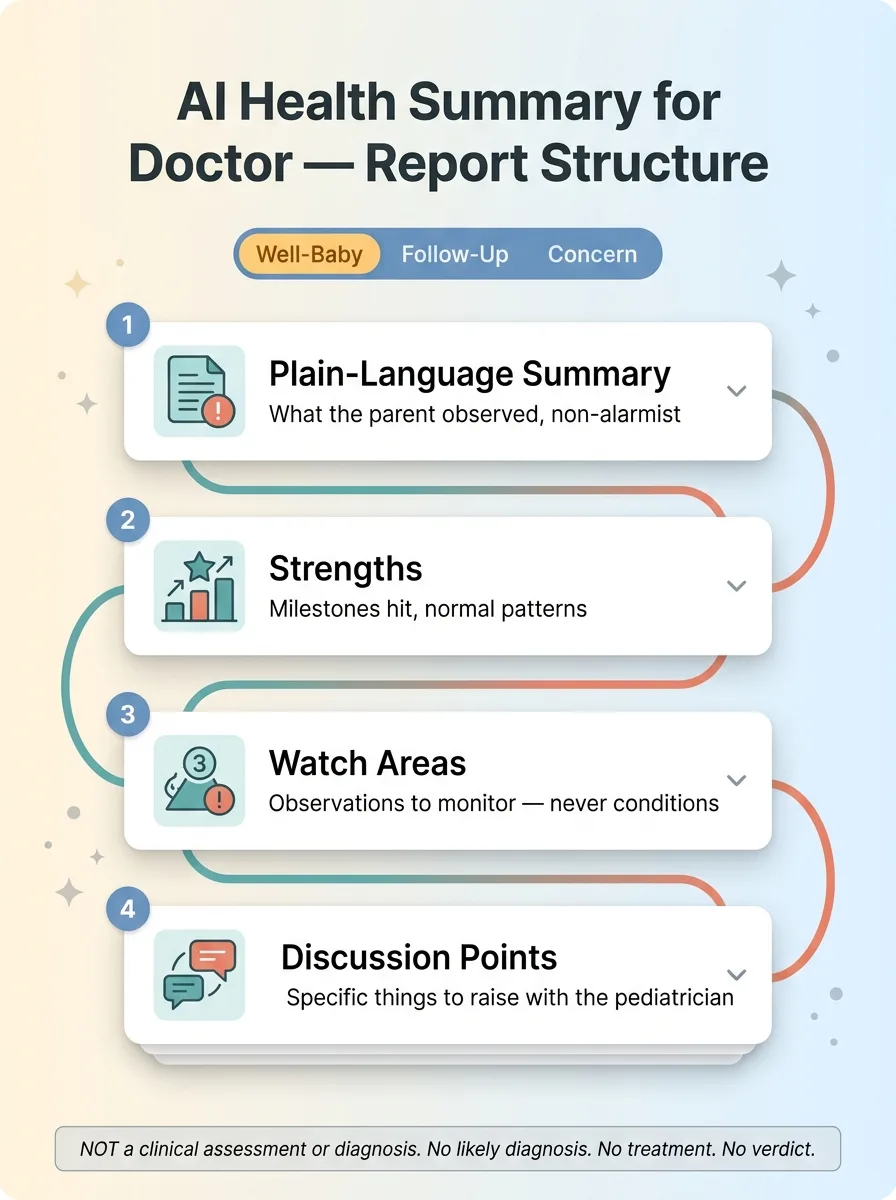
It generates visit-type-specific reports. A well-baby check is a different document than a follow-up, which is different from a parent bringing a specific concern. The structure adapts to the context of the visit, because what you want to communicate to a pediatrician changes depending on why you're there.
Visit-type-specific reports
A well-baby report leans toward development and routine observations. A follow-up report centers on what changed since last time. A concern report organizes the specific thing the parent is worried about into a clear timeline. Each one renders as expandable cards, so the parent (and the clinician) can scan the headline and drill in only where it matters.
Four sections every report has
No matter the visit type, every report has the same four parts:
 Anatomy of the parent pre-visit report
Anatomy of the parent pre-visit report
- A plain-language summary of what the parent observed, written in clear, non-alarmist language
- Strengths, the things going well, milestones hit, normal patterns worth noting
- Watch areas, observations worth keeping an eye on, framed as observations, never as conditions
- Discussion points, the specific things to raise with the pediatrician
Notice what's not in there. There's no "likely diagnosis." No "recommended treatment." No verdict anywhere.
The output is deliberately written as the parent's own notes, in the parent's voice, to hand to the pediatrician. It reads like the well-prepared parent every clinician wishes they had. Not like a competing medical opinion the doctor has to argue with.
That framing matters more than it looks. The structure mirrors how a busy clinician actually wants information delivered: top-line first, organized, with the questions explicit. It turns a chaotic 15 minutes into a focused one.
For the parent, it turns 20 minutes of late-night worry into an organized page they can actually use. The instinct everyone has is to make AI smarter about the child. The thing that actually helps is making the parent more organized.
The framing is the product: how the disclaimer does real work
This is the part most teams miss, so I want to be exact about it.
 AI proposes, human disposes, division of labor
AI proposes, human disposes, division of labor
The disclaimer is not legal boilerplate stapled on at the end. The disclaimer is the product spec.
The report states explicitly that it is not a clinical assessment or diagnosis, and that the pediatrician should use it alongside their own evaluation. That single framing decision is not a defensive afterthought. It dictates everything upstream.
Once you commit to "this is the parent's organized notes, not a medical opinion," every other choice follows. The prompts change. The section names change. I call them discussion points, not recommendations, because the parent isn't recommending a course of action, they're flagging what to talk about. I call them watch areas, not symptoms-of-concern, because the parent is observing, not diagnosing.
The tone changes too. The whole thing is written to inform a conversation, not to pre-empt one.
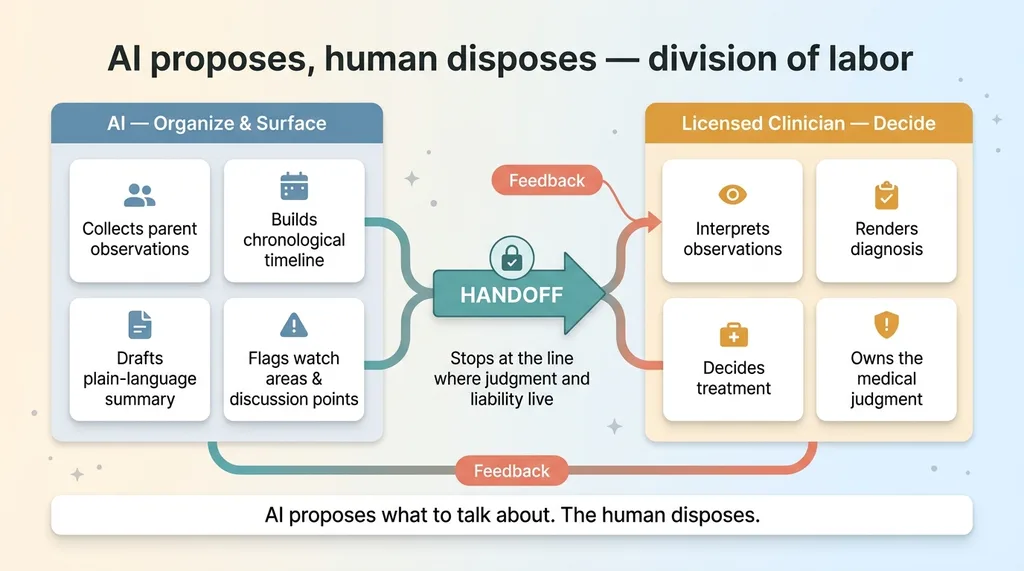
The principle underneath: the AI proposes what to talk about, the human clinician disposes. The model surfaces and organizes. The licensed human decides what it means. That's not a compromise I made to stay safe. It's the correct division of labor, and it happens to also be the safe one.
This is the same pattern in every AI system I ship, it stops for a human. The AI does the work it's good at, then hands off at the exact point where judgment and liability live.
Here's what I'll tell you that took me a while to internalize. Getting the framing right is harder than the model work. Anyone can prompt a model to summarize symptoms. Drawing the line between "organize the parent's observations" and "assess the child" with enough precision that it holds across thousands of generated reports, in tone, in structure, in every word choice, that's the actual engineering. The model is the easy part.
How to tell if a health AI use case is safe to build
Here's a test you can apply to your own ideas without a lawyer in the room. Three questions.
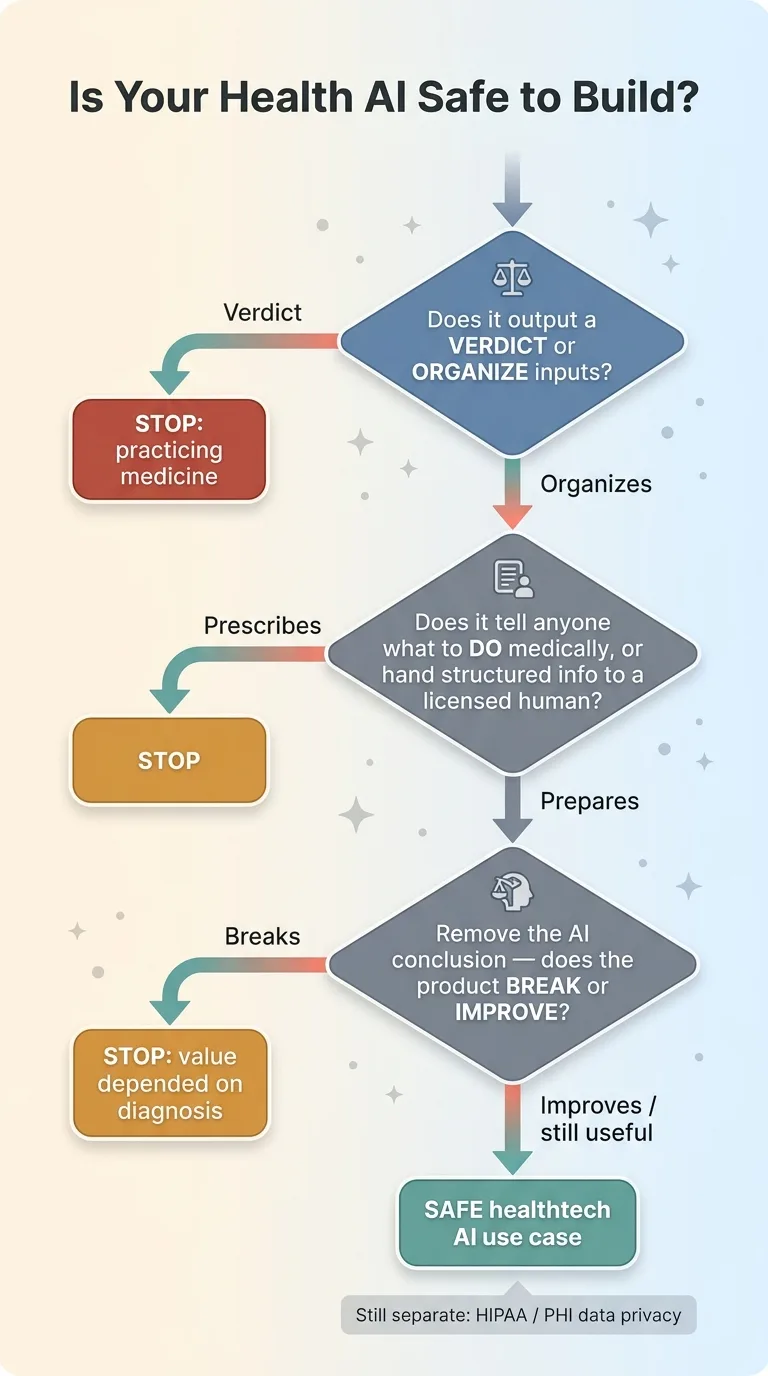 Three-question safety test decision tree
Three-question safety test decision tree
Does the AI output a verdict, or does it organize inputs? If the output is a conclusion the user didn't already supply, you're generating clinical judgment. If the output is the user's own information, restructured, you're organizing. Organizing is safe. Concluding is not.
Does it tell anyone what to do medically, or does it hand structured information to a licensed human? "You should take X" is a problem. "Here are the things to ask your doctor about" is not. The first prescribes. The second prepares.
Does removing the AI's conclusion break the product, or improve it? This is the cleanest test. Strip out every clinical judgment your AI makes. If the product collapses, your value depended on practicing medicine, and you have a problem. If the product gets cleaner and still useful, you've probably found a safe healthtech ai use case.
In my parent-summary feature, you can remove every shred of clinical judgment and the product is exactly as valuable. That's not an accident. It's the test, applied during design.
One honest caveat. This rule keeps you out of the practicing-medicine trap. It does not solve data privacy. PHI handling, HIPAA, where the data lives, who can see it, how it's stored, that's a separate problem with its own requirements. "Safe from a clinical-liability standpoint" and "compliant with health data law" are two different boxes, and you need to check both.
Finding the safe spot in your own regulated business
This pattern is not a pediatrics thing. It's a regulated-industry thing.
Organize, don't assess. AI proposes, humans decide. Framing as the product, not as a disclaimer bolted on later. I've built this exact shape into financial advisory, into HR compliance, into labor compliance SaaS. The same pattern shows up in every regulated industry I touch, because the underlying constraint is the same: a licensed human has to own the judgment, and the AI's job is to make that human faster and better prepared.
The hard part is never the model. The model is a commodity now. The hard part is drawing the line in exactly the right place: far enough that the AI is genuinely useful, short of where it starts making decisions that a licensed professional has to legally own.
Too cautious and you ship something that doesn't help anyone. Too aggressive and you've built a liability that one bad output can detonate.
Finding that line is the work I do as a Chief AI Officer. Not the prompt engineering. The judgment about where AI is both safe and worth shipping in a business where being wrong has real consequences.
If you've got a regulated use case and you're not sure where that line is, or you've been burned by a vendor who didn't care to find it, that's exactly the conversation I want to have.
Thinking about AI for your business?
If this resonated, let's talk. I do free 30-minute discovery calls where we look at your actual operations and find where AI could move the needle, and just as important, where it shouldn't go.
Get AI insights for business leaders
Practical AI strategy from someone who built the systems — not just studied them. No spam, no fluff.
Hodgen.AI
Ready to automate your growth?
Book a free 30-minute strategy call with Hodgen.AI.
Book a Strategy Call