Marketing Consent vs HIPAA Consent: Don't Mix Them
Marketing consent vs HIPAA consent: why bundling them causes TCPA and FTC fines, and how to build an audit-grade consent ledger that keeps them separate.
By Mike Hodgen
The $9 Million Lesson Hiding in Your Signup Flow
Two numbers should keep every health-brand founder up at night: $1.5 million and $7.8 million.
The first was an FTC settlement involving a well-known prescription-discount company. The second hit a well-known online therapy platform. Both are public regulatory record. And neither was a hack.
There was no breach, no stolen database, no hooded figure in a basement. These were normal-looking marketing setups. Someone wanted to retarget signups on Facebook. Someone wanted to measure ad conversions. So they dropped a pixel, synced an audience, and called it growth marketing.
The problem is what flowed through those pipes. Health intent, diagnoses, prescription data, the kind of thing a person told the company in confidence ended up in an ad platform. The legal core of both cases was the same: consent for one thing got treated as consent for everything.
If you run a longevity, telehealth, or any health-adjacent DTC brand, the question you're actually asking is blunt: am I one pixel or one bad checkbox away from a six-figure settlement?
I want to be honest with you up front. The fix here is not exciting. It's not a vendor product with a dashboard. It's structural, it's boring, and it's the kind of thing that looks like overkill right up until a regulator asks you to prove something you can't prove.
The confusion that creates this exposure is almost always the same. Founders treat marketing consent vs HIPAA consent as if one is just a heavier version of the other. They're not. They're two completely different legal animals living in two different legal homes, and when you stack them onto one checkbox, you collapse two compliance regimes into a single liability.
Let me walk you through the distinction, the three ways teams blow it, and the structural fix I'd build if you handed me your signup flow today.
Marketing Consent vs HIPAA Consent: Two Different Legal Animals
People assume these sit on a spectrum. Marketing consent is the casual one, HIPAA consent is the serious one, and if you get the serious one you've covered the casual one. That mental model is exactly how brands end up in FTC filings.
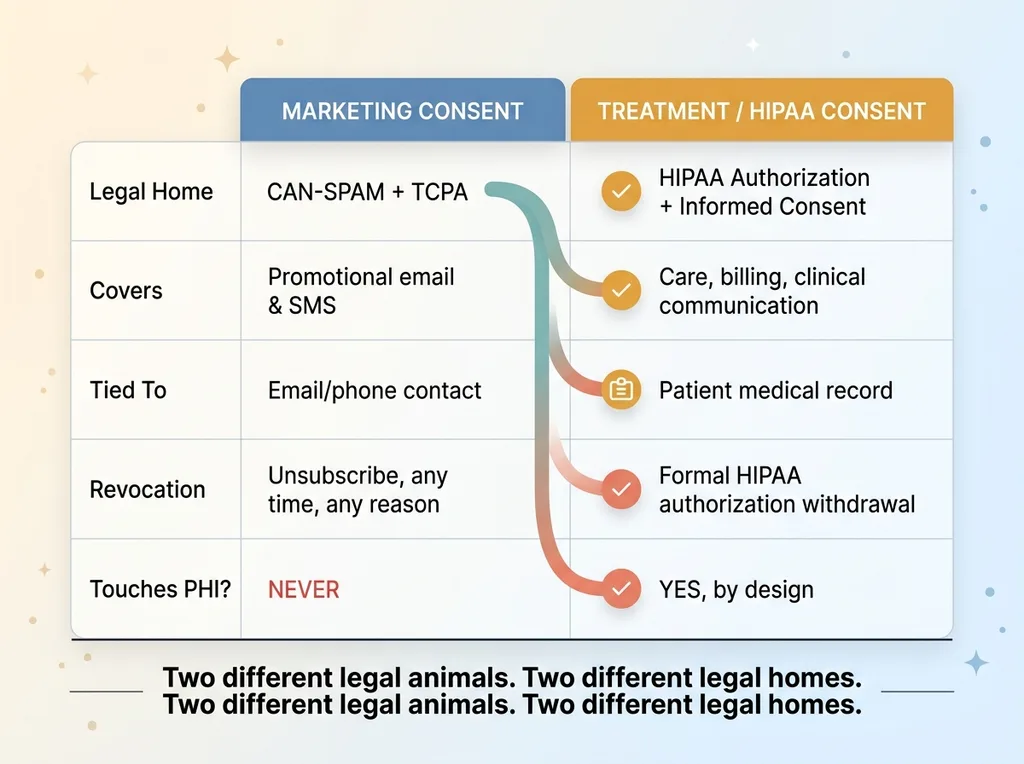 Marketing Consent vs HIPAA Consent side-by-side comparison
Marketing Consent vs HIPAA Consent side-by-side comparison
They are not stronger and weaker versions of the same permission. They live in different statutes, follow different revocation rules, and cover different data.
What marketing consent actually governs
Marketing consent lives under CAN-SPAM and TCPA. It covers promotional email and promotional SMS. It is revocable at any time, by the person, for any reason. And it should never, under any circumstance, touch protected health information.
TCPA in particular treats SMS as its own beast. You can't fold text-message consent into a general "keep me updated" box. The law expects explicit, unbundled opt-in for SMS, with the exact consent language logged at the moment the person agrees. Not paraphrased later. The actual words they saw.
Think of a longevity telehealth brand. Someone lands on the site, likes the pitch, and wants the newsletter. That's marketing consent. It governs the right to send them a promo for a new peptide protocol. Nothing more.
What treatment consent actually governs
Treatment consent is a different document entirely. It's a HIPAA authorization plus informed consent, tied to the patient record. It governs care, billing, and clinical communication.
When that same longevity prospect books a consult, completes intake, and becomes a patient, they sign something that lets the provider treat them, bill them, and message them about their care. That authorization is anchored to their medical record. It does not expire because they got annoyed by a marketing email.
Here's the load-bearing point. These two consents have different legal homes, different revocation mechanics, and different data scopes. A marketing unsubscribe and a HIPAA authorization withdrawal are not the same action and should never trigger each other. The moment you treat them as one permission, you've built a single point of failure across two regulatory frameworks.
How Mixing Them Creates Exposure (The Three Failure Modes)
In practice, the damage almost always comes from one of three quiet defaults. Each one feels convenient. Each one is a fine waiting to happen.
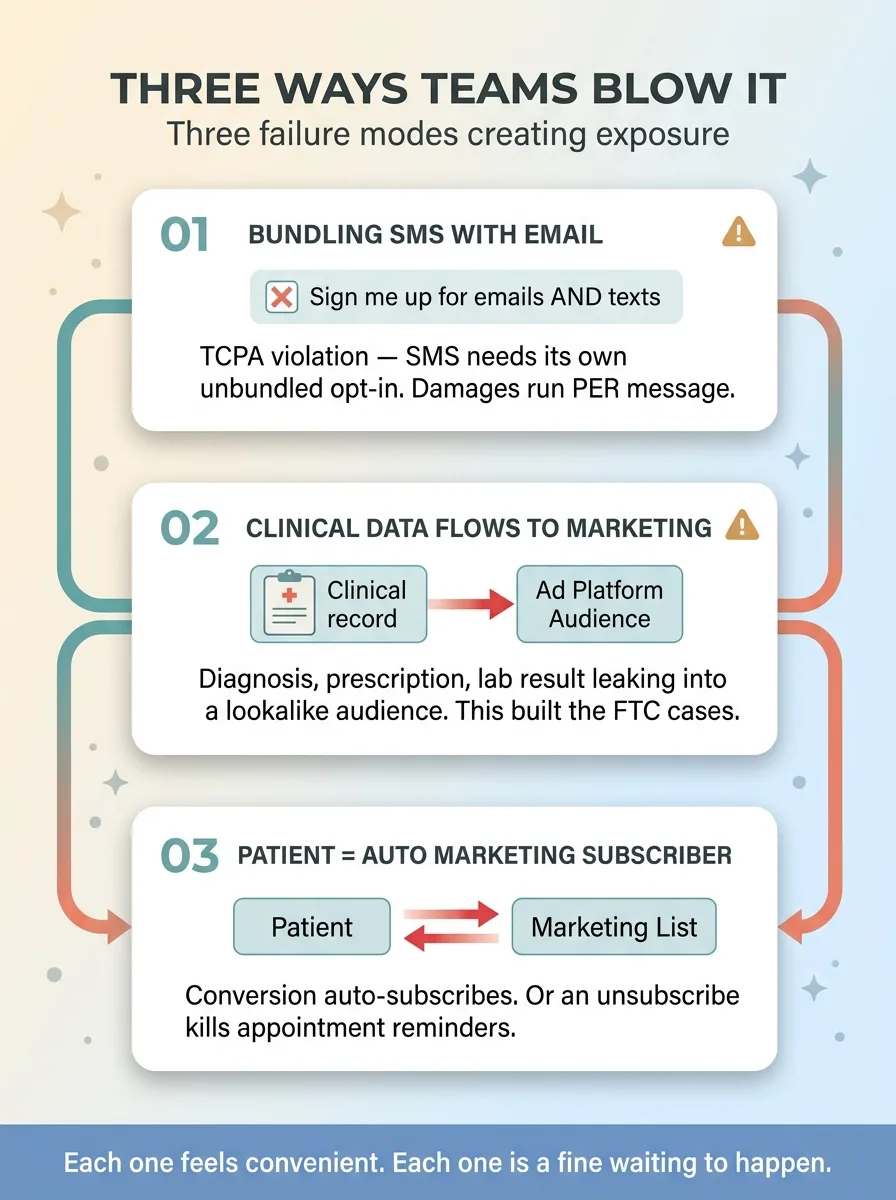 The Three Failure Modes that create exposure
The Three Failure Modes that create exposure
Bundling SMS consent with email consent
You've seen the checkbox: "Sign me up for emails and texts." It's everywhere. It's also a straight TCPA problem.
SMS consent has to be its own explicit, unbundled opt-in. When you bundle it with email, a person who only wanted your newsletter is now legally considered to have not properly consented to texts, because they never made a separate, affirmative choice about SMS. TCPA damages run per message. Multiply that across a list and the math gets ugly fast.
Letting clinical data flow back into the marketing list
This is the one that built the public FTC cases. A diagnosis, a prescription, a lab result, even the fact that someone searched for a specific condition flows back into a marketing audience or an ad-platform custom audience.
That's the exact mechanism. Someone tells your telehealth brand they're being treated for a hormone issue, and weeks later that data point is sitting inside a lookalike audience on an ad network. I wrote about how the tracking pixel that fined two health companies $9M made this happen at the technical level, and the short version is: the pixel didn't know the difference between a marketing event and a clinical one. Nobody told it.
Treating a patient as an automatic marketing subscriber
The third failure mode runs in both directions. You convert a marketing lead into a patient, and your system auto-adds them to the promotional list. Now their patient relationship is being used as implied marketing consent it never was.
Or the reverse: someone unsubscribes from your marketing emails, and that unsubscribe also kills their appointment reminders. Now you've used a marketing action to disrupt clinical communication, which is a care problem on top of a compliance problem.
Each of these is a default someone chose because it was easy. None of them was malicious. All of them are structural cracks.
The Fix Is a Consent Ledger, Not a Checkbox
The solution isn't a better checkbox. It's a consent ledger. And the design of that ledger is where the real protection lives.
Start with the principle that every consent is its own event with its own rules.
One direction only: marketing to clinical
SMS consent gets its own event. Unchecked by default. Timestamped. The exact consent language captured verbatim at the moment of opt-in. Never bundled with email. Never inferred from a patient relationship.
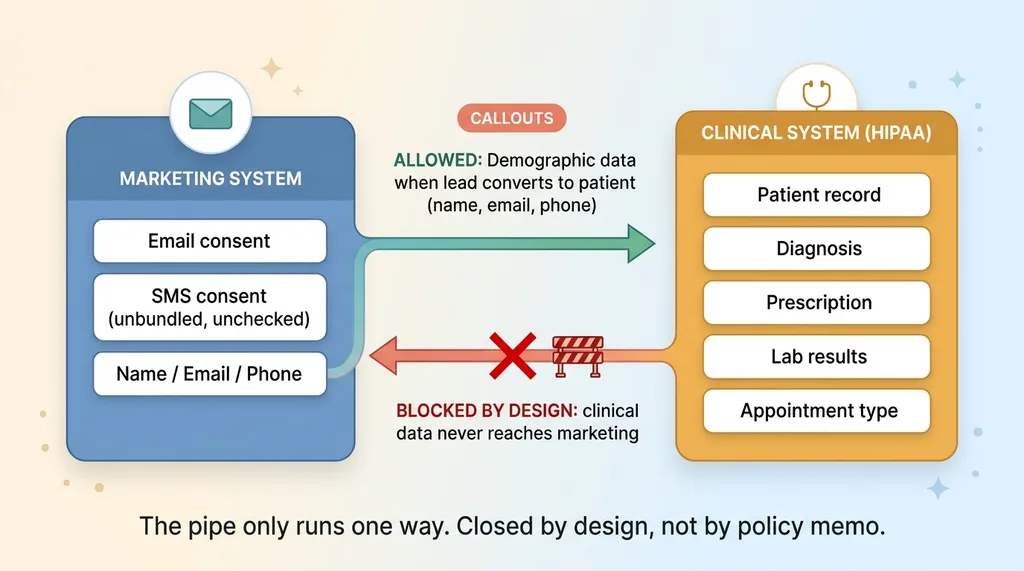 One-directional data flow between marketing and clinical systems
One-directional data flow between marketing and clinical systems
Treatment consent lives in a completely separate store, tied to the patient record, governed by HIPAA authorization rules.
Then you enforce a one-directional data rule, and this is the part that actually prevents the FTC scenario. Demographic data (name, email, phone) can flow marketing-to-clinical when a lead converts to a patient. That makes sense. You need to know who your patient is.
But clinical data never flows back to marketing. Not the diagnosis. Not the prescription. Not the appointment type. Not the lab result. The pipe only runs one way, and the clinical-to-marketing direction is closed by design, not by policy memo.
Separate stores, separate revocation
The two consents live in separate systems with separate revocation logic. I go deeper on this in my piece on separating marketing and treatment consent, but the rules are simple to state and hard to fake.
Converting to a patient does not auto-subscribe anyone to marketing. Unsubscribing from marketing does not stop care messages. A HIPAA authorization withdrawal does not touch the marketing list, and a marketing unsubscribe does not touch the patient record.
This is deliberately boring architecture. It doesn't demo well. There's no slide that makes a board gasp. But it's the difference between "we can prove our setup keeps these regimes separate" and "we hope nobody asks."
What an Audit-Grade Consent Record Has to Capture
When a regulator asks you to prove consent, "we have a record somewhere" is not an answer. You need a ledger that holds up under scrutiny. Here's what every consent event in that ledger has to capture.
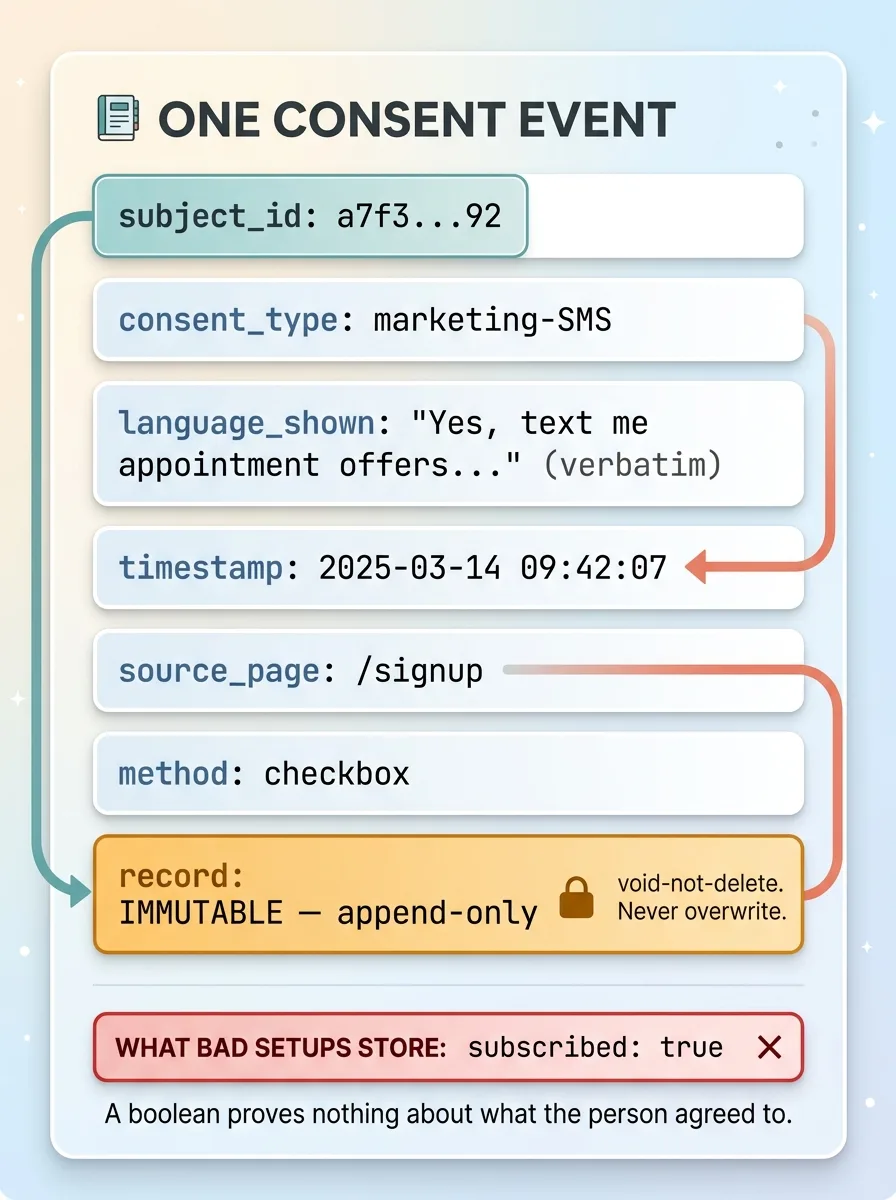 Anatomy of an audit-grade consent ledger record
Anatomy of an audit-grade consent ledger record
- A unique subject identifier so you can tie the event to a person without dumping their whole profile into the log
- The consent type: marketing-email, marketing-SMS, or treatment authorization, kept as distinct categories
- The exact language shown at that moment, stored verbatim, not a reference to "current terms" that may have changed five times since
- A timestamp down to the second
- The source and page where the consent was given
- The method: checkbox, signature, or verbal-logged
- An immutable record that can't be edited after the fact
That last point matters more than it sounds. The rule is void-not-delete, append-only. You never overwrite a consent event. If someone changes their mind, you append a new event. The history stays intact.
Here's the test the whole thing has to pass. A regulator says, "Prove this person agreed to receive texts on this date." You should be able to produce the exact words they saw, the timestamp, and the method, in seconds. If you can only produce "they're on our SMS list," you've already lost.
Storing this well also forces you to keep the clinical side isolated, which is its own discipline. The less PHI you hold and the tighter you scope it, the smaller your blast radius if anything goes wrong. I cover that approach in shrinking your HIPAA footprint.
Let me be honest about why this matters so much. Most fast-built signup flows don't capture exact language and don't keep these events separate. They store a boolean. "subscribed: true." That's it. When an audit hits, that's exactly where they find blood, because a boolean proves nothing about what the person actually agreed to.
How I'd Stress-Test a Health Brand's Consent Setup Today
If you handed me your telehealth or longevity brand's signup flow right now, I could find your exposure in about 30 minutes with six questions.
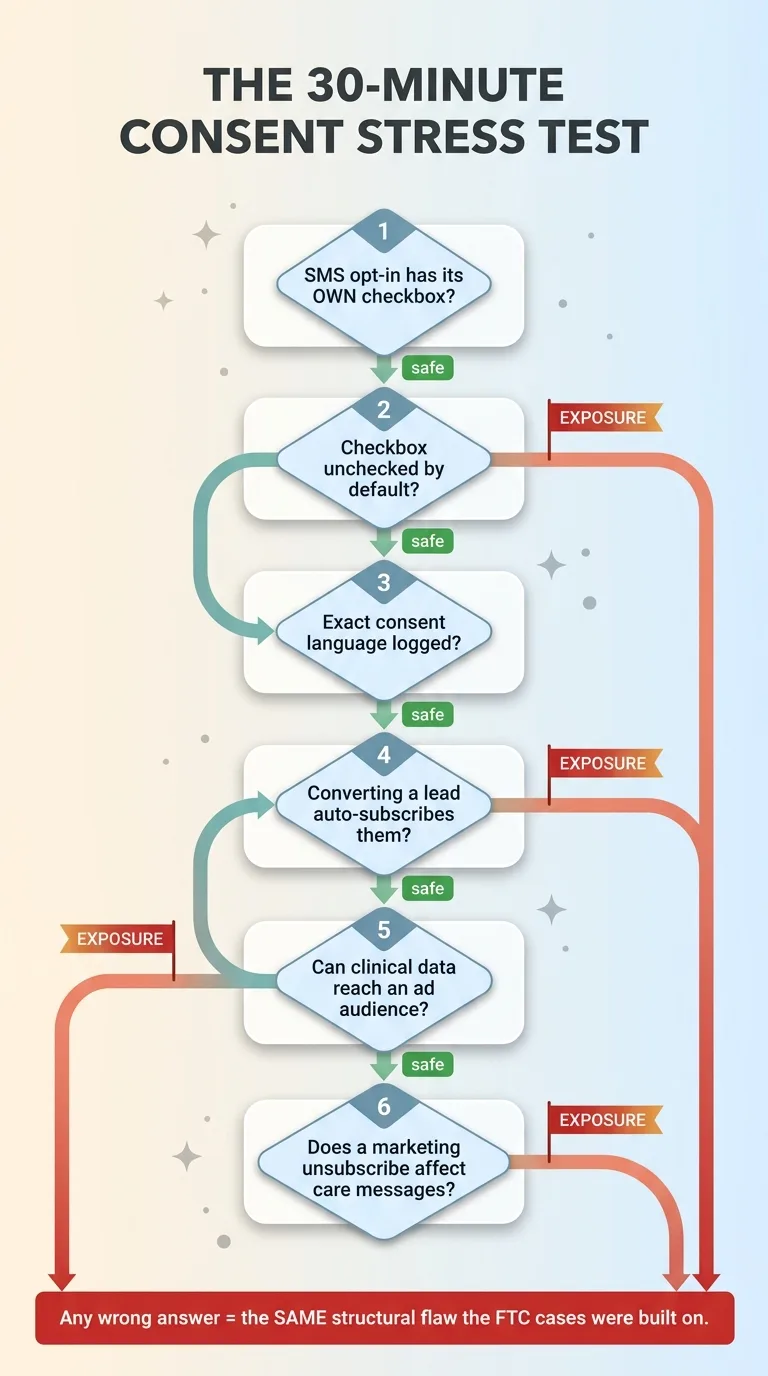 Six-question consent stress-test decision flow
Six-question consent stress-test decision flow
Does your SMS opt-in have its own checkbox, separate from email?
Is it unchecked by default?
Do you log the exact language the person saw when they opted in?
Does converting a lead into a patient auto-subscribe them to anything?
Can clinical data, a diagnosis, a prescription, an appointment type, reach an ad platform's custom audience?
Does a marketing unsubscribe affect appointment reminders or any clinical message?
Any "yes" to the wrong one of those is the same structural flaw the public FTC cases were built on. Not a similar flaw. The same one.
Now let me reframe the fear I named at the top. You're probably not one pixel away from a settlement by accident. The companies in those cases weren't reckless. But you might be one default away, one bundled checkbox, one helpful auto-subscribe, one pixel that fires on a clinical event because nobody told it not to.
And here's the part that should make you feel better, not worse: the fix is design work, not a lawsuit. It's a consent ledger, separate stores, and a one-directional data flow. It's boring, it's buildable, and it's a lot cheaper than $7.8 million.
I build this separation correctly the first time, with the ledger and the one-directional flow baked in from the start, instead of bolted on after a regulator comes knocking. If you want a second set of eyes on where your setup actually stands, have me audit your consent flow and I'll tell you straight where the cracks are.
Ready to bring AI leadership into your company?
I work with a small number of companies at a time. If you're serious about AI, apply to work together and I'll review your application personally.
Get AI insights for business leaders
Practical AI strategy from someone who built the systems — not just studied them. No spam, no fluff.
Hodgen.AI
Ready to automate your growth?
Book a free 30-minute strategy call with Hodgen.AI.
Book a Strategy Call